The End-of-Life Battle Over Jewish Souls

Image by Lily Padula

By Paul Berger October 14, 2014
Sylvia Sodden lay on life support in a critical care room in Brooklyn when her health care proxy made the hardest choice: He decided to end her life.
But before any machines could be unplugged, her relatives turned to Chayim Aruchim, a program that helps ultra-Orthodox Jews navigate end-of-life care. Chayim Aruchim referred the family to a lawyer who obtained a temporary restraining order against the proxy.
Days later, a Brooklyn Supreme Court judge replaced the proxy with Sodden’s older sister.
According to Halacha, or Jewish law, every moment of life is precious. The judge’s decision was handed down this past March. Sodden, 78, remained on life support for six more weeks.
Moshe Borowski, Chayim Aruchim’s director of outreach and education, noted in a publicity article about Sodden’s case that those additional weeks translated into 3,628,800 seconds. “Can we even begin to calculate the value of more than 3.6 million seconds?” Borowski asked.
Borowski wrote in the article, published in May, that Sodden chose her proxy “during a period of particularly great duress.”
What Borowski omitted was that Sodden had converted to Catholicism 60 years earlier. Her health care proxy was not, as Borowski implied, a random “gentleman from her neighborhood.” He was her godson, Joseph Arrigo, a high school math teacher from Connecticut.

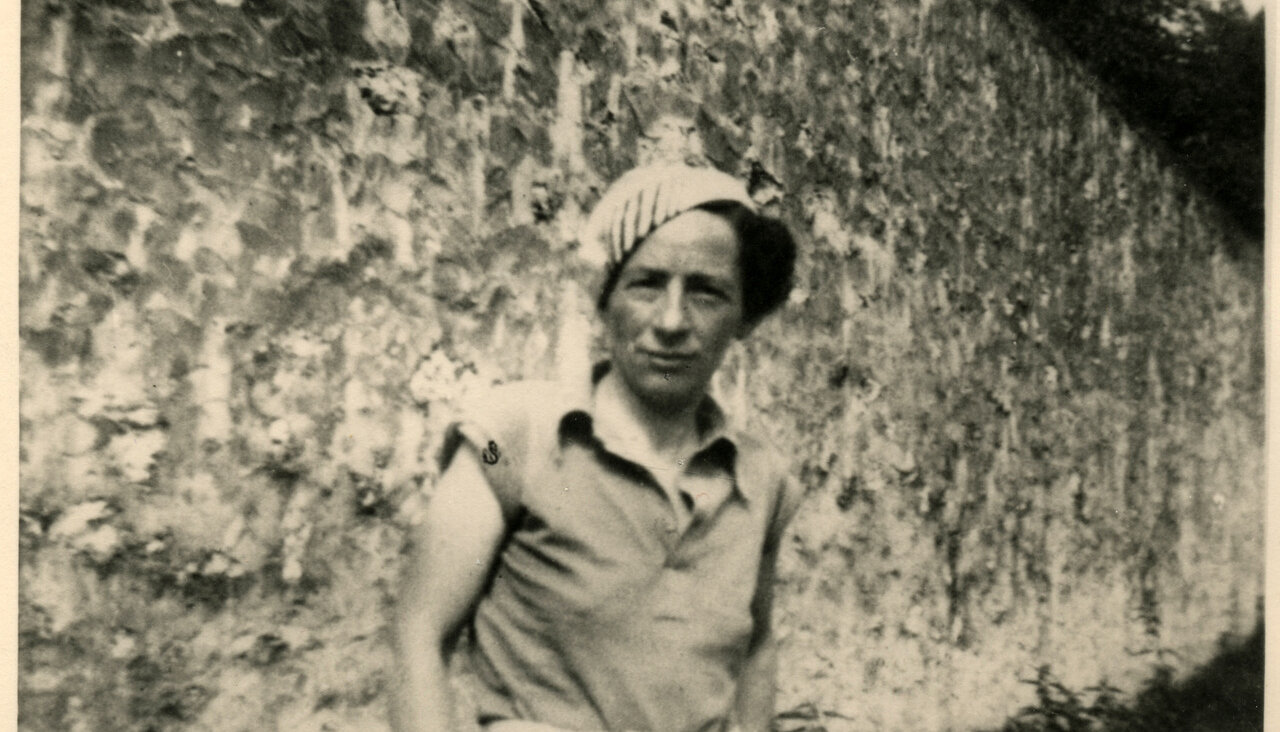
Godparents: Sylvia Sodden sits with Joseph Arrigo on her knee following Joseph’s baptism in 1960. The gentleman is Arrigo’s uncle and godfather, Joe Rosati. Image by Courtesy of Joseph Arrigo
Arrigo told the Forward that Sodden chose him as her proxy because she believed that only Arrigo would honor her wish not to be kept alive on “tubes and machines.”
Arrigo said, “Sylvia didn’t want to live that way.”
•
Many Orthodox Jews, particularly ultra-Orthodox Jews, believe that as long as the heart beats, the soul is alive. For such Jews, withdrawing life support is akin to murder.
Rabbi Shmuel Lefkowitz, vice president of community services at Agudath Israel of America, an ultra-Orthodox group, said that a few years ago his organization received a spate of calls from families complaining about doctors who wanted to remove brain-dead patients from life support.
During the same period, Lefkowitz said that Agudath Israel also became concerned about pending legislation in New York State that required doctors to discuss palliative care options with terminally ill patients. The bill’s authors believed that the Palliative Care Information Act would ensure that patients were offered the option of a more dignified, less painful death. But in Agudath Israel’s eyes, the bill was one more step in society’s march toward helping people to die instead of treating them.
“The Agudah is the 800-pound gorilla that sits where it wants to.”
Agudath Israel launched Chayim Aruchim in 2010 in response to both of these issues, Lefkowitz said.
Chayim Aruchim’s finances are modest. According to its first tax filing, in 2012, the group raised $16,000 in contributions and spent $4,000. But Chayim Aruchim is a program of Agudath Israel, which has tens of millions of dollars in assets and wields considerable political power in states with significant Orthodox populations. At Chayim Aruchim’s most recent annual meeting a few weeks ago, the group’s board talked of expanding to England, Canada and Israel.
In just a few short years, Chayim Aruchim has persuaded the North Shore LIJ Health System, which includes Lennox Hill Hospital, to alter its end-of-life protocols for brain-dead patients. Previously, brain-dead patients were kept on a ventilator for up to 72 hours. Today, families who claim a moral or religious exemption can request that brain-dead patients remain on a ventilator until their heart stops, which can take days or, in extreme cases, weeks, months or years.
Chayim Aruchim also persuaded New York State legislators to amend the Palliative Care and Information Act so that in addition to palliative care, doctors in the state must also discuss patient options for aggressive care.
“The Agudah is the 800-pound gorilla that sits where it wants to,” said Nancy Dubler, a consultant for ethics at New York City Health and Hospitals Corporation. “They have the political power to make people hone to their position.”
Dubler, a professor emerita at Yeshiva University’s Albert Einstein College of Medicine, said she agrees with Agudath Israel’s view that life is precious. But there are times when continuing life “is such a burden for the patient that in secular terms it’s unjust and unfair.” She said she has no problem with individuals who choose more aggressive treatment or less analgesia in order to remain conscious to the end. “But to impose that on someone who can’t choose is where I am uncomfortable,” Dubler said.
•
Sodden’s is not the only case this year in which a patient’s end-of-life wishes have been challenged on religious Jewish grounds. In September, Morton Avigdor, the same lawyer who overturned Sodden’s health care proxy, filed a petition in Brooklyn Supreme Court in the case of Eileen Kramer, a 60-year-old developmentally disabled woman who was on life support at Brooklyn’s Maimonides Medical Center.
Avigdor represents the Hebrew Academy for Special Children, which runs an adult residential home where Kramer has lived for the past 40 years.
HASC’s director, Samuel Kahn, claimed in his petition that Kramer’s legal guardian, her brother Howard Kramer, had instructed Maimonides to withdraw life-supporting treatment. “This must be stopped at all costs,” Kahn stated in court papers, first reported by DNAinfo. “Having known Ms. Kramer for many years, I know that she would not want her life to be ended by being denied life support. She is an Orthodox Jew.”
But Howard Kramer told the Forward that he and his sister were raised in a Reform Jewish household. Besides, Kramer said, his sister’s developmental disability, which includes severe cognitive limitations, has prevented her from ever being able to grasp the concept of being religious, let alone Orthodox.
Kramer flew to New York from his home in Denver in mid-September when his sister became critically ill. Doctors recommended withdrawing life support. Initially, Kramer agreed. But he began to receive calls from people associated with HASC, “some of them very self righteous and strident” telling him that every moment of life is precious and that he must keep his sister alive as long as possible.
Kramer said he was grateful to HASC for looking after his sister so well. As a compromise, he agreed to keep his sister on life support, as long as other aggressive, life-extending procedures were discontinued. Kramer thought HASC had accepted the compromise. He said he felt blindsided when HASC took him to court.
Kramer said HASC falsely claimed in its petition that he had asked Maimonides to withdraw life support. (The hospital, citing HIPA laws, would not comment.) He was most offended that HASC claimed in court papers that he had little contact with his sister and that he “does not understand [her] wishes.” Kramer said that he used to speak to his sister regularly by phone and that he visited New York, on average, twice a year. He said HASC’s own files describe him as a “devoted” brother.
“I really see it as dishonest,” Kramer said. “On top of the whole situation, to have somebody say that is really outrageous.”
•
Chayim Aruchim is, in many ways, a response to a shift in medical ethics. During the past 20 years, physicians have increasingly come to question the value of Western medicine’s ability to keep patients alive — in pain and suffering — with no chance of improvement. “I think the goal of medicine is to sustain the patient’s life and to make the patient’s life better,” Dubler said. “I certainly don’t think it’s the goal of medicine to extend organ function for a patient who is no longer capable of making decisions, when extending that organ function causes pain and suffering for no benefit.”
The philosophy of dying a “good” death is anathema to many Orthodox Jews.
This philosophical shift mirrors a dramatic growth in palliative care during the past decade. Palliative care, which focuses on improving a patient’s quality of life, can be practiced alongside curative treatment or on its own. According to the Center to Advance Palliative Care, between 2000 and 2012 the number of palliative care teams at medium-sized and large hospitals almost tripled, from 658 to 1,734. The reduction of pain and stress has been shown in some cases to extend life. But palliative care can also involve the use of morphine, which can shorten life.
A recent nonpartisan report commissioned by the Institute of Medicine found that dying patients are often put through needless, aggressive treatment when they would have been better off with palliative care in a hospice or at home. The report, “Dying in America,” cited “perverse financial incentives” for hospitals to pursue aggressive treatment. It recommended that insurers pay physicians to consult patients early on and regularly about their wishes for end-of-life care.
The philosophy of dying a “good” death is anathema to many Orthodox Jews who believe that life should be sustained at all costs. In a 2005 court case involving a disagreement over the insertion of a feeding tube into a Jewish woman’s stomach, a Queens Supreme Court justice noted that “the first halachic principle of medical intervention is that whenever it is possible to increase the longevity of a patient, it should be done.” Judge Martin Ritholtz added that Orthodox rabbis are divided on how much a person should be allowed to suffer and for how long. One prominent rabbi, Moshe Feinstein, believed that it is not obligatory to aggressively treat a dying person who is in pain and is suffering. But Ritholtz noted that another influential rabbi, Eliezer Waldenberg, believed that “suffering serves to increase a person’s merit, and therefore prolonged suffering is a good reason to prolong life, in order to erase sins and to allow the person an opportunity to repent.”
The emphasis on preserving life at all costs is not a uniquely Jewish value. Christian, Muslim and secular families may have myriad moral, ethical and religious reasons to reject palliative care or to pursue aggressive treatment to the end. In many cases, physicians themselves are reluctant to give up treatment, even after it has become obvious that the patient is dying.
But if clergy do become involved in end-of-life issues, they are most likely to be Orthodox rabbis, Dubler says. Agudath Israel places great emphasis on involving rabbis in end-of-life issues. Its Halachic Medical Directive, hosted on Chayim Aruchim’s website, has a section for people to select a rabbi whose guidance their health care proxy should follow. In a recent letter to The New York Times, Agudath Israel’s director of public affairs, Avi Shafran, wrote that “decisions about when, if ever, to give up on [life] are the province of patients and their religious advisers, not graduates of medical schools.”
Doctors in New York and New Jersey, home to large Orthodox communities, often consult directly with rabbis to discuss treatment options and outcomes. The rabbi uses that information to issue guidance on which course of treatment is permissible according to Jewish law. Many families, particularly ultra-Orthodox families, will abide by that decision.
Most frequently, when disputes arise, they involve artificial hydration, feeding and pain management. Palliative care and medical ethics specialists with decades of experience in New York City hospitals told the Forward they have seen many cases of Orthodox patients who are put through aggressive treatments or denied pain medication because of a rabbi’s ruling.
“I think too often [Orthodox rabbis] elect to prolong life because they believe in prolonging life per se, regardless of the dignity of the individual,” said Kenneth Prager, chairman of the medical ethics committee at Columbia University Medical Center.
Prager said he has seen dying Orthodox patients endure uncomfortable procedures because of a desire to prolong life, even for a short period, regardless of the consequences. These include patients who suffer severe fluid retention and total body swelling, painful skin ulcerations, and repeated needle sticks and catheter insertions as part of their treatment.
Not only is such treatment uncomfortable for the patient, but it can be distressing for family members, too. Prager said he has seen Orthodox families lament prolongation of life at all costs, but they “ruefully accept the rabbi’s ruling, even though it hurts them.”
•
Sylvia Sodden loved the sun. In the spring of 2011, her godson drove 70 miles from his home in Fairfield, Connecticut, to visit her at Sea Crest Rehabilitation and Health Care Center, in Brooklyn. Sodden had moved into the nursing home 10 years earlier when she became wheelchair bound. She did not go out often, and Arrigo liked to a pick warm day for his infrequent visits so that he could take her along the boardwalk at nearby Coney Island. Arrigo would sit on a bench. Sodden would sit in her wheelchair, her eyes closed, her face tilted toward the sky.
This particular day, as they sat on the boardwalk, Sodden told Arrigo that the nursing home had asked residents to choose a health care proxy in case there came a time when they could no longer make their own medical decisions. Sodden told Arrigo that she did not want to be kept alive on tubes and machines. She said that she wanted him to be her health care proxy. Her form stated: “My agent knows my wishes regarding artificial nutrition and hydration.”

On the Boardwalk: Joseph Arrigo loved to take his grandmother Sylvia Sodden (seen here in 2007) for walks along the boardwalk at Coney Island, Brooklyn. Image by Courtesy of Joseph Arrigo
“I said, ‘Why pick me? You have brothers and sisters,’” Arrigo recalled. “She said, ‘Because I think you could follow through.’”
Sodden chose her sister, Esther Feigenbaum, as her alternate proxy.
Sodden was born in January 1936, into an Orthodox Jewish home in Brooklyn. Her father, Isaac Sodden, was a pulpit rabbi. She had many brothers and nephews who were also Orthodox rabbis. “Our family is a deeply religiously committed Orthodox Jewish family,” Feigenbaum wrote in an affidavit earlier this year.
According to Arrigo, Sodden converted to Catholicism on Christmas Day 1957, at St. Francis Xavier Roman Catholic Church, in Manhattan. (St. Francis Xavier does not have a record of her baptism on that date in 1957 or in surrounding years.) Sodden chose Gloria Arrigo, a colleague and friend from her job at Guardian Life Insurance Company of America, to be her godmother. When Gloria gave birth to her first son, Joseph, a few years later, she asked Sodden to be his godmother.
Sodden never married, and she had no children of her own. Joseph Arrigo said she relished the role of godmother. She took him to restaurants, plays and movies. She was his sponsor at his confirmation. After Arrigo grew up and moved to Connecticut, he maintained a close relationship with her. He called her every week or two and visited as often as he could, making sure never to miss January 12, Sodden’s birthday. He also gave Sodden money toward two religious pilgrimages she made to Lourdes, France, and to pay for extra comforts when she moved into Sea Crest. “I enjoyed treating her well to, in some way, give back to her some joy considering all that she did for me my whole life,” Arrigo said in a written statement submitted as part of the court case this year. “I believe in my heart that I succeeded in doing this.”
Sodden suffered breathing problems in August 2013. She was transferred to Coney Island Hospital. When Arrigo visited a few weeks later, Sodden had already been placed on a ventilator and a feeding tube. She was slipping in and out of consciousness. By October she was uncommunicative. Arrigo placed his finger inside hers and asked her to squeeze. There was no response.
Arrigo said that in October, doctors at Coney Island Hospital met with him and several members of Sodden’s family, including her sister, Feigenbaum. The doctors suggested that a tracheotomy might help Sodden to breathe more easily. Arrigo said he acceded to the tracheotomy request “partly out of respect for Sylvia’s family.” Sodden’s condition stabilized, and in December she was transferred to Four Seasons Nursing & Rehabilitation Center, but she remained unconscious.
This past January a doctor examined Sodden at Arrigo’s request. The doctor found that Sodden was “in a vegetative state with no sign of cognitive functioning or capability.” Arrigo called Feigenbaum to say that he wanted to exercise his proxy and remove life support. “I remember distinctly there was stone silence on the phone,” Arrigo said.
When Arrigo called Four Seasons, he said he was told that the home was run under Jewish auspices and that they would not remove life support. Four Seasons also said that its ethics board had to review Sodden’s case before it would allow her to be transferred to a hospital to die. (Four Seasons did not respond to questions about its policy on ending a patient’s life.) Before that meeting could take place, Arrigo received a call from Four Seasons saying that Sodden had experienced a medical problem during dialysis and had been transferred back to Coney Island Hospital.
Arrigo recalled that at a meeting at Coney Island Hospital a doctor pleaded with Sodden’s relatives to consider removing life support. The doctor said Sodden was probably in pain and that there was no chance of recovery. But the family would not budge. Arrigo said he vividly recalls how Feigenbaum’s son-in-law “barged into the room late and said, ‘Are we going to kill her?’”
Arrigo said he asked Feigenbaum’s husband, Samuel Feigenbaum, “if we could wave a magic wand and Sylvia came awake and communicative for one minute, and suppose she said, ‘I want these machines — everything — taken off me. I want to move on to my next life.’ I asked, ‘What would you do?’ He said, ‘I would tell her she would have to stay on the machines and the feeding tube.’”
Arrigo said he agonized over the decision to withdraw Sodden’s life support. He said he had great respect for her family’s religion, but he felt bound by Sodden’s request to him to be her proxy. He sought guidance from two Catholic priests. “It’s just a very difficult thing to do,” Arrigo said.
In March, Arrigo decided to act. Feigenbaum had stopped taking or returning his calls, so he called Coney Island Hospital and asked them to prepare to withdraw life support. He asked the hospital to inform Sodden’s family. That was when Avigdor, the attorney, acting on Feigenbaum’s behalf, called Arrigo.
Avigdor called on a Wednesday, Arrigo recalled. He asked him not to “do anything drastic” before a doctor could be flown in from Israel to assess Sodden’s condition on the following Monday or Tuesday. Arrigo agreed, but he warned Avigdor that he needed “to make a move soon, because she is suffering.”
On the Monday, Arrigo received an email from Avigdor saying a temporary restraining order had been taken out preventing him from withdrawing life support, and that there would be a court hearing the following morning in Brooklyn.
Arrigo was at work when he received the email. He did not notice that the attached legal document also threatened to remove him as Sodden’s health care proxy and to instate Feigenbaum in his place.
At the court hearing the following day, March 18, Feigenbaum submitted an affidavit stating that her sister had a 60-year history of mental health problems, including schizophrenia and bipolar disorder. She said Sodden was not mentally competent to sign a health care proxy in 2011. Feigenbaum stated that rather than being in a vegetative state, her sister was “awake and in and out of awareness, and can continue to be a living, conscious adult with a right to remain living.”
“According to our Jewish values, it is imperative that my sister be permitted to remain on life support and that she be permitted to live,” Feigenbaum said. She added: “The family strongly believes that she would want to continue living, even on life support.”
Arrigo missed the court hearing; he said it was too short notice to take the day off work. Shortly after 12 p.m. he called the courthouse. A clerk told him that he had been removed as Sodden’s proxy.
Arrigo felt that he had been duped. Avigdor’s email correspondence and phone conversations never mentioned removing Arrigo as health proxy. Worse, Arrigo thought Sodden’s family was forcing her to endure unnecessary pain and suffering that she had specifically stated she wanted to avoid. “I think it’s morally and ethically wrong to stomp on someone’s personal wishes,” Arrigo said.
The following day, he rushed to Brooklyn to file an appeal.
•
As far as many New York doctors are concerned, Chayim Aruchim is a solution, not a problem. Orthodox Jews turn to rabbis for direction on many aspects of life, from keeping the laws of kashrut to business disputes and personal problems. Since many families trust rabbis far more than they trust doctors, Chayim Aruchim gives them the confidence to make end-of-life choices, including the fraught decision to forgo a ventilator or a feeding tube. Columbia’s Prager said: “I thought Chayim Aruchim existed in part to alleviate some of these problems and to confront Orthodox families with the inevitability of death and not keeping someone alive as long as possible.”
But Chayim Aruchim’s website tells a different story. Its message is that hospitals too often withhold treatment to keep down costs and mortality rates. The site links to news stories that highlight people who survived after they were thought to be dead or in a vegetative state. It hosts a Wall Street Journal article showing how hospitals are reducing mortality rates by keeping patients with a poor prognosis out of intensive care units. It also hosts a New York Times article questioning the cost of dialysis for elderly patients who are dying.
Lefkowitz spoke of some of these issues at a conference organized by Chayim Aruchim in 2011. He told attendees that before a patient is transferred to an ICU, doctors evaluate the patient’s prospects. According to Hamodia, an ultra-Orthodox newspaper that summarized (but did not quote from) Lefkowitz’s talk, Lefkowitz said that if doctors believe that recovery in the ICU is unlikely, “the recommendation is made that the patient be discharged, thus depriving him of possible lifesaving treatment.”
At the same conference, Rabbi Zvi Ausch, Chayim Aruchim’s halachic adviser, told attendees that if a doctor gives a bleak prognosis, it is important to get a second opinion. “It’s unfortunately common today that [doctors] don’t say the real truth,” Ausch said, according to a recording on Chayim Aruchim’s website. “You know, they give a very hopeless outlook despite in the back of their minds, if it would be a close relative to them, they probably would not talk like this.”
Ausch also commented on a case study involving an 83-year-old woman with advanced dementia who was admitted to hospital with a range of life-threatening conditions. Ausch said that it was not up to the woman’s health care proxy, her son, to decide how she should be treated. “The decision-making process belongs to the Ruv,” Ausch said.
In an email to the Forward, Lefkowitz said that Chayim Aruchim has put many families in touch with rabbis who have, “where the Halacha permits,” advised patients or their families to sign a DNR — a do not resuscitate order —to enter hospice or to take pain medication. “Pain medication is not per se prohibited by Halacha,” Lefkowitz added. “The dosage needs to be monitored.”
Some doctors say that on a case-by-case basis, ultra-Orthodox rabbis can be more flexible than their public pronouncements. Beth Popp, director of palliative medicine at Maimonides, said: “I don’t think I’ve ever met a rabbi who is pro suffering. They usually want us to be attentive to pain and other symptoms patients have, and to try and alleviate unnecessary suffering.” Rabbi Charles Rudansky, director of pastoral care at Metropolitan Jewish Health System, a palliative care group, said: “They don’t want to be known as the rabbi that allows DNR. However, on one-to-one cases their responses will be much different and palliative.”
Ultra-Orthodox Jews are particularly resistant to hospice care because of Halacha’s emphasis on extending life. But Rudansky, who is Modern Orthodox, said that Chayim Aruchim guides many of his ultra-Orthodox patients to MJHS. “They are the linchpin,” Rudansky said. “If I say something or a nurse says something, it won’t mean anything. They have to get a stamp of approval from their halachic authorities.”
MJHS is one of the largest hospice and palliative care organizations in New York State, and it has close ties to Chayim Aruchim. Lefkowitz is chairman of the board of MJHS Foundation, which raises and allocates funds to MJHS and its related programs. Lefkowitz also led the creation of MJHS’s “Halachic Pathway” initiative, which guarantees that a rabbi will guide an Orthodox patients’ treatment and hospice care.
Even so, Rudansky said Chayim Aruchim treats MJHS cautiously. Rabbis advise patients to withdraw from hospice if their care is deemed to violate Jewish law. “They kind of hold the hand of the individual and say, be on guard,’” Rudansky said.
The Forward asked to speak to Ausch, Chayim Aruchim’s chief halachic adviser, to better understand how Chayim Aruchim weighs aggressive care and pain management in relation to Jewish law. Lefkowitz said that Ausch does not give interviews. Instead, Lefkowitz put the Forward in touch with Eliezer Gewirtzman, a 35-year-old ultra-Orthodox rabbi from Lakewood, New Jersey, who is one of six rabbis listed as active in Chayim Aruchim’s program.
Gewirtzman said he struggles with questions regarding DNR orders and pain management. He told of a recent case in which a family did not want their relative to be given morphine for fear that it would shorten the patient’s life. Gewirtzman reassured the family that the morphine would not shorten life if it were administered in the correct way, so they followed his advice. “What they need to hear from me is that the pain relief they are taking… is a track that is taking into consideration their belief that hours and minutes count,” Gewirtzman said.
Gewirtzman receives about one call a week about end-of-life issues, mostly from families with questions related to dementia or to end-stage cancer. He was educated at Beth Medrash Govoha, a huge yeshiva in Lakewood. But he said that he has always had a fascination with medicine. During the past couple of years, he has attended seminars organized by Chayim Aruchim in which physicians such as palliative care and critical care doctors, oncologists and cardiologists, discuss the risks and benefits of feeding tubes, ventilators, pain management and other treatments so that Gewirtzman can apply that knowledge to Jewish law.
“We can’t just allow such a patient to wither away.”
Gewirtzman said his overriding goal is the continuation of life. This means that in some cases where physicians might want to withhold treatment, Gewirtzman might recommend continued treatment. He described a recent case in which a family approached him about a hospital that was reluctant to insert a feeding tube into a dying, 93-year-old woman suffering from dementia. Gewirtzman put the woman’s family in touch with a specialist in gastroenterology who works with Chayim Aruchim. The specialist advised that the woman would survive the procedure, so the woman’s family demanded it. “Although a patient is sick and although a patient is demented, we can’t just allow such a patient to wither away without feeding them,” Gewirtzman said. The woman died of other complications before the tube could be inserted.
•
Arrigo applied to be reinstated as Sodden’s proxy on March 19. One week later, Justice Lawrence Knipel moved his court to Sodden’s bedside at Coney Island Hospital. “She was observed to be an elderly woman breathing without distress, her hands swollen and possibly fidgeting, her mouth moving with her lips opening and closing,” Knipel noted in his decision, published a couple of weeks later. “She seem[ed] unresponsive to moderate verbal or physical stimuli. Although not observed by this Court, there is reason to believe that Ms. Sodden opens her eyes occasionally and may shudder at loud noise.”
In a nearby conference room, Knipel heard medical testimony that Sodden had end-stage kidney disease and that although she was not brain-dead, she was “not conscious, uncommunicative and unresponsive.”
Feigenbaum testified that she had never spoken to her sister about Sodden’s end-of-life wishes. But she restated her belief that Sodden was not mentally competent to sign a health care proxy, and that even if Sodden was mentally competent she remained Jewish, so removing life support would contradict “her religious and moral beliefs.”
Arrigo represented himself at the hearing. He testified that Sodden suffered from bipolar disorder, not schizophrenia. He added that although she suffered mental breakdowns about once every 10 or 12 years, with the help of medication she lived “a happy, humorous, well-adjusted, fully functional and independent” life. He provided evidence that during the 1980s Sodden was a parishioner of Our Lady of Angels Roman Catholic Church, in the Bay Ridge section of Brooklyn. She also regularly received a Holy Communion wafer at Sea Crest.
Knipel delivered his ruling April 3. He said there was no evidence that Sodden was mentally incompetent at the time she signed the proxy. He added that Arrigo, “an articulate person sensitive to [Feigenbaum’s] religious beliefs, cannot be said to be acting in bad faith in acting on what he has reason to believe was [Sodden’s] wishes.” Knipel reinstated Arrigo as Sodden’s health care proxy. The same day, Feigenbaum filed an appeal.
Arrigo maintained constant contact with Coney Island Hospital as he waited for the appeals court decision. By the third week of April, Sodden’s doctors told him that she had only a few days to live. On April 29, the appeals court denied Feigenbaum’s appeal. Sodden died the following day, before Arrigo had a chance to ask the hospital to remove life support.
Arrigo said that he felt as though he had let Sodden down. “My only hope is she really didn’t suffer all those months,” he said.
Feigenbaum declined to speak to the Forward. “We’ve had quite enough publicity about this,” she said.
The Forward suggested to Lefkowitz that Chayim Aruchim misrepresented Sodden’s case in Borowski’s articles that appeared in Orthodox media, Hamodia and the 5 Towns Jewish Times. Over several emails, Lefkowitz stuck to Chayim Aruchim’s narrative, that Sodden was “not of sound mind when she purportedly signed the document.” When the Forward pointed out that the courts found in Arrigo’s favor, Lefkowitz directed further questions to Avigdor.
Avigdor said Sodden’s family maintains that she was not mentally competent to sign the health care proxy. He said the family does not accept her conversion to Catholicism, because she was “not in her right mind” then either. Avigdor added that if he had had more time, he could have gathered medical evidence of her mental illness. She was “clearly a very troubled woman,” he said.
Avigdor also said that if Sodden had converted to Catholicism, the ramifications for her family would have been huge. “A woman who converts does not get buried in a Jewish cemetery,” Avigdor said. “She is separated forever from her family.”
The Forward suggested to Avigdor that there was no evidence that Sodden had schizophrenia, and that people with mental illness lead full lives. What if Sodden was of sound mind when she converted? What if her health care proxy was a reflection of her wishes? “You’re assuming she had wishes that would be respected and that she thought about it and was competent to make those decision,” Avigdor said. “The family position was — and it is very well grounded — she didn’t know what she was doing. She was a mental patient.”
Sea Crest specializes in physical and occupational therapy. It is not a mental health facility.
•
Sodden was buried in a Jewish cemetery. But when Arrigo wants to honor her, he drives out to Lourdes in Litchfield, a replica of the grotto in France where pilgrims pay tribute to St. Bernadette.
When Sodden died, Arrigo made a “sizable donation” in her name toward the renovation of a modest chapel at Lourdes in Litchfield. In the next few months, a plaque naming all the donors will be mounted in the chapel there. Sodden’s name will be among them. Arrigo said Sodden had a special connection to St. Bernadette, who is famous for a series of visions she had in 1858, culminating in a vision of the Virgin Mary. Nonbelievers thought she was mentally ill. The Catholic Church made her a saint.
Contact Paul Berger at [email protected] or on Twitter, @pdberger

Did you know that only 2% of Forward readers donate to support our nonprofit newsroom? That 2% make it possible for millions to read the Forward without a paywall or subscription — removing any barriers to the full and fair Jewish story.
But while the Forward is free to read, it isn’t free to produce. Big stories — like deep dives into the antisemitism data, political scoops or reporting trips to college campuses — take months of research and fact-checking. All while we keep you informed of what you need to know each day.
— Rachel Fishman Feddersen, Forward Publisher & CEO
Support our mission to tell the Jewish story fully and fairly.